
Every telehealth business runs on five core workflows — and the quality of the software managing those workflows determines whether the business scales or stalls. Disconnected tools create manual handoffs at every stage. Integrated platforms eliminate them. The difference shows up in patient LTV, churn rates, and operator margin — not in marketing claims. ⚠ Disclaimer: This article is for informational purposes only and does not constitute medical or legal advice.
The Five Workflows That Run a Telehealth Business
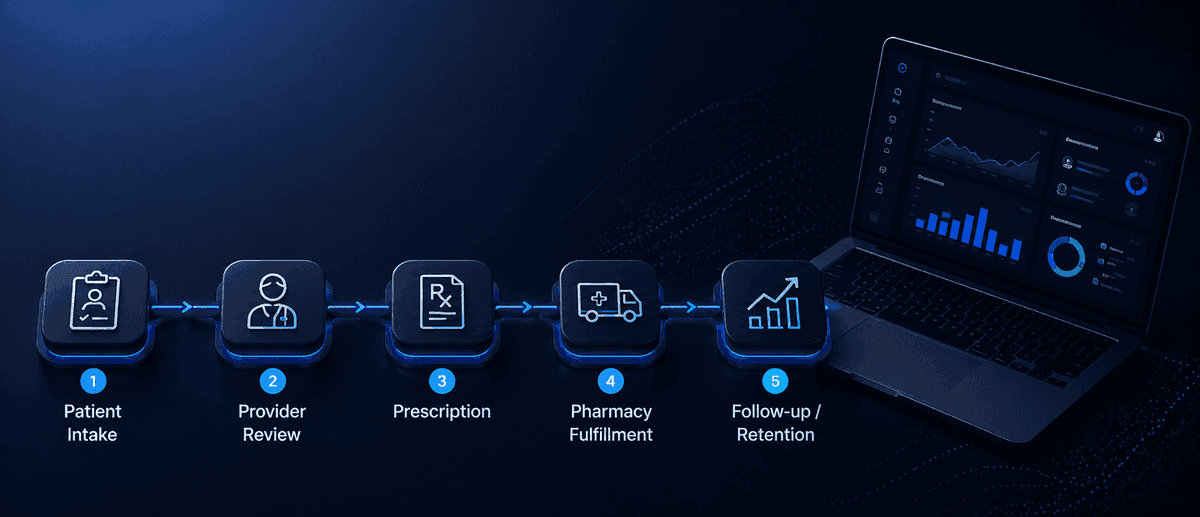
Every telehealth program — regardless of clinical category or operator type — is governed by the same five operational workflows. How well these workflows are built and connected determines operational scalability and patient retention.
1. Patient Intake. The collection of demographic data, medical history, and clinical consent that begins every patient relationship. Poor intake design creates three compounding problems: inconsistent data quality that slows provider review, incomplete consent documentation that creates compliance exposure, and patient frustration from poor UX that drives pre-clinical abandonment.
2. Clinical Review. A licensed provider evaluates the intake submission and makes a prescribing decision. This is the only workflow that cannot be automated — clinical judgment requires a licensed clinician. Everything surrounding it (case routing, documentation, notification) can be automated. The workflow design determines how many cases a provider can review per day and how consistent that review quality is across the patient population.
3. Pharmacy Fulfillment. The prescription is transmitted to the pharmacy partner, compounded or filled, and shipped to the patient. The connection between this workflow and the clinical review step — whether it is automated or manual — determines fulfillment reliability, which directly affects retention.
4. Subscription and Payment Management. Recurring billing, renewal processing, failed payment retry, and subscription status management. Involuntary churn from billing failures is one of the most preventable losses in a subscription health business.[1]
5. Patient Communication. Automated notifications at each stage — intake confirmation, provider review complete, prescription sent, shipment tracking, refill reminder, renewal confirmation. Communication quality directly affects patient confidence in the program and willingness to continue subscribing.
Where Manual Workflows Create Business Risk
Manual workflows fail in three predictable ways as patient volume grows — and the failure modes are specific enough that operators can anticipate them before they occur.
Intake failures compound at volume. A manual intake review process that handles 20 submissions per day without issue becomes a bottleneck at 100 per day. Inconsistent eligibility screening creates compliance gaps. Slow triage creates intake abandonment patients who completed the questionnaire but did not hear back within their expected window and moved on.
Pharmacy coordination failures are the most expensive in terms of patient relationship cost. A manual prescription routing process introduces transcription errors, missed fax confirmations, and lost prescription events. Each failure requires operator intervention, creates a delay, and produces a patient support interaction that damages program trust. For subscription programs with monthly refill cycles, one pharmacy failure can cost a patient who was on track to generate 12 months of subscription revenue.
Billing failures without automated retry logic produce involuntary churn — subscription lapses that were never intended by the patient. Industry research suggests 20–40% of total subscription churn in digital health is involuntary.[1] Automated retry sequences and payment update prompts recover the majority of these lapses before they become cancellations.
Integrated vs Disconnected Workflow Tools
Many early-stage telehealth operators assemble their workflow stack from disconnected tools: a form builder for intake, a scheduling or telemedicine tool for providers, a separate pharmacy portal, and a CRM layered on top. This approach feels flexible at launch and becomes expensive to maintain by the time the business reaches 300–500 patients.
Disconnected tools create integration debt: custom connections between systems that require engineering maintenance, break when components update, and create data inconsistencies when patient records exist in multiple places.
More critically, disconnected tools create operational handoffs at the most failure-prone points in the patient journey. When intake completes, someone or something must transfer that case to the provider. When the provider approves a prescription, someone or something must transmit it to the pharmacy. When the pharmacy ships, someone or something must update the patient and the subscription system.
Integrated workflow platforms eliminate these handoffs. When intake completes, the case routes to the provider queue automatically. When the prescription is approved, pharmacy transmission fires automatically. When fulfillment completes, the subscription system triggers the next refill cycle automatically. The operator's role shifts from managing workflows to managing the business.
How Each Workflow Affects Patient LTV
Patient LTV in a subscription telehealth program is not determined solely by clinical outcomes — it is determined by the smoothness and reliability of the operational experience across all five workflows.
Patients who receive their treatment on schedule, with clear communications at each stage, with their subscription renewing without friction, stay subscribed longer than patients who experience delays, gaps, or billing confusion — even when clinical outcomes are identical.
The data on this is consistent across subscription health businesses: fulfillment reliability correlates strongly with retention, independent of program efficacy.[2] Patients equate a smooth operational experience with a trustworthy program. Operational failures break that trust in ways that are difficult to recover from.
This means the ROI of workflow automation is not purely a cost reduction calculation — it is also a revenue protection calculation. Every manual workflow that has a failure mode is a LTV risk at scale.
Workflow Infrastructure in FUSE Health
FUSE Health is designed as an integrated workflow platform for non-clinical operators. Every stage of the patient journey — from intake through subscription renewal — is connected in a single system with automated handoffs between stages.
Intake submissions route to provider queues automatically. Approved prescriptions transmit to pharmacy partners automatically. Fulfillment updates return to patients automatically. Refill cycles initiate based on configurable program logic. Subscription billing and retry sequences run without operator intervention.
Operators configure program parameters — subscription cycle, refill timing, pricing — and the platform manages execution at any patient volume. The result is a telehealth program that scales with patient volume, not with operations headcount.
Conclusion
Healthcare workflow software is the infrastructure that separates scalable telehealth operations from businesses held together by manual coordination. The five core workflows — intake, clinical review, pharmacy fulfillment, subscription management, and patient communication — determine patient LTV, operator margin, and whether the business scales or stalls at the first volume inflection point.
FUSE Health provides integrated workflow infrastructure for non-clinical operators who want to launch and scale prescription wellness programs without building or managing disconnected operational tools.
References
[1] Profitwell (Paddle), "The State of Subscription Churn in Digital Health," 2024. profitwell.com
[2] McKinsey & Company, Consumer Health Survey and Digital Health Retention Research, 2024.
McKinsey & Company Consumer Health Survey (2024)
- American Telemedicine Association Operational Framework Guidance (2024)
- FDA Digital Health Compliance Guidance (2024–2025)
- Wheel Virtual Care Industry Report (2024)
- HIMSS Telehealth Workflow Optimization Research (2024)
- Rock Health Digital Health Consumer Adoption Report (2024)

Daniel is a two-time founder who has scaled service businesses across major U.S. markets. A Y Combinator competition winner, he focuses on removing operational and regulatory barriers so operators can build and scale modern healthcare businesses.
- Background
- Startup Operations & Service Systems
- Experience
- 2x Founder, Multi-Market U.S. Scaling
- Qualifications
- Healthtech Market Expertise & Operational Scaling
- Key Achievement
- Scaled Premier Staff & Eventstaff across major U.S. markets



